Root Canal Therapy
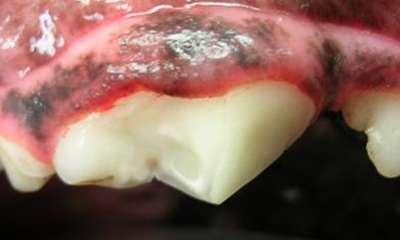
Root canal therapy is a far less invasive and painful option to save fractured or discolored teeth than surgical extraction.
KEY FACTS
- Root canal therapy is a procedure that is used to save functionally important teeth like
- Grasping/retrieving teeth
- Canine teeth
- Large chewing teeth in dogs
- Canine teeth in cats
- The therapy includes an oral examination under anesthesia, teeth cleaning/polishing, dental x-rays, and sterilization of the root canal, sealing of the root canal and composite restoration.
QUICK LOOK


LEARN MORE
Root canal therapy is a far less invasive and painful option for fractured tooth or discolored tooth than surgical extraction. The goal is to treat the tooth before it becomes infected or painful. Moreover, root canal therapy allows your pet to retain the tooth for functions like grasping/retrieving or chewing.
Working dogs (police, herding, hunting, obedience) obviously need their teeth for their “job” or “use”. Many receive root canal therapy and most are supported with a titanium crown when a tooth or teeth are damaged. Root canal therapy is also the preferred treatment for our zoo patients.
